 LINGCORE SCI
LINGCORE SCI
The Synthetic Control Method: Constructing Counterfactuals for Single-Unit Health Policy Evaluation
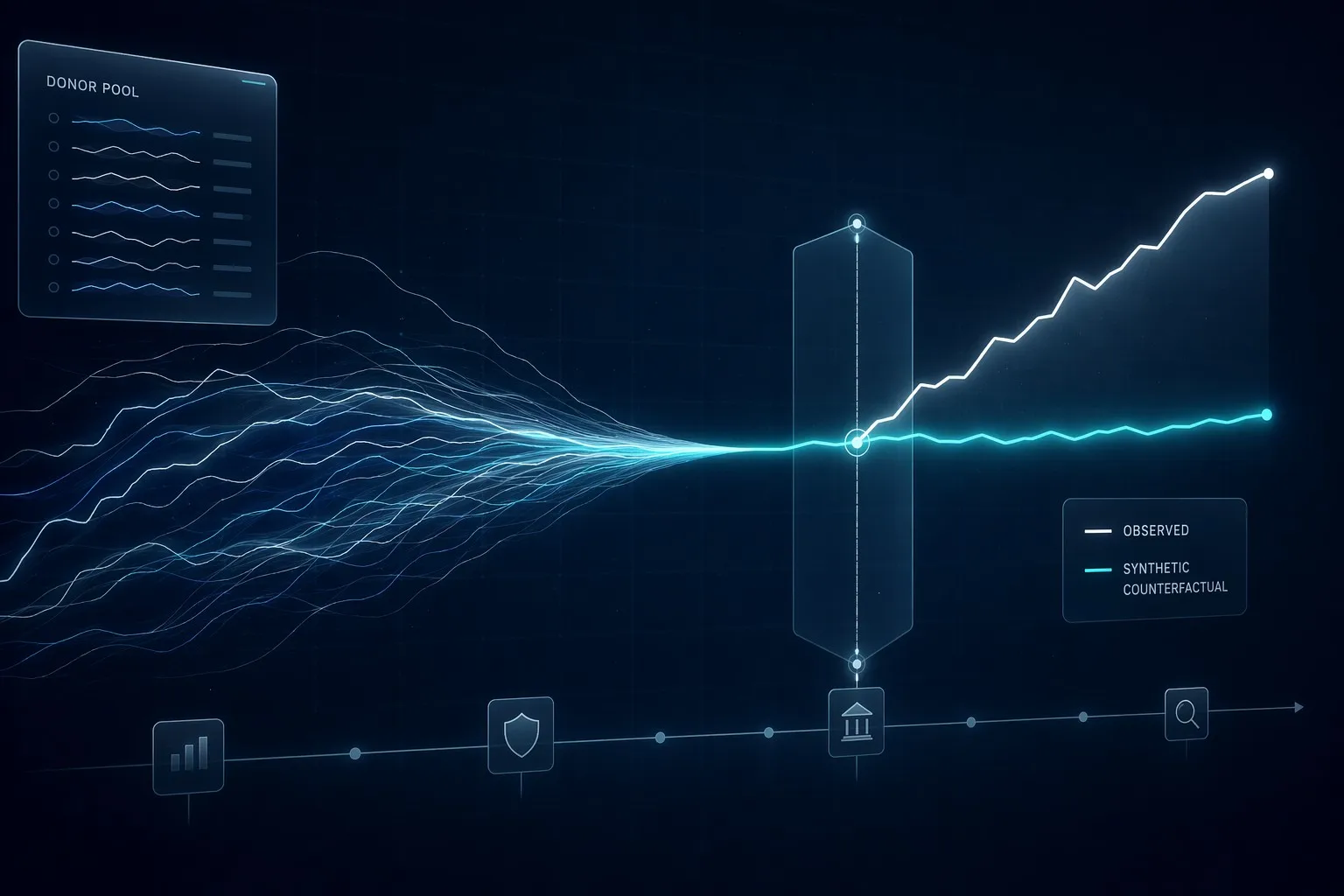
The Synthetic Control Method (SCM) constructs a weighted combination of untreated comparison units (a "donor pool") to build a data-driven counterfactual for a single treated unit — such as one state, hospital system, or country — when no natural comparison group exists. The pre-intervention fit between the synthetic control and the treated unit is the primary indicator of credibility, validated through placebo-in-space and placebo-in-time tests.
Health policy interventions frequently occur at an aggregate level that leaves researchers with only one treated observation. A single state expands Medicaid eligibility. A single hospital system implements a new sepsis protocol. A single country adopts a national vaccination mandate. In each case, there is exactly one treated unit and no obvious individual-level comparison group, because the intervention was never randomized and applies uniformly to an entire jurisdiction.
Traditional difference-in-differences designs require a plausible parallel-trends assumption relative to a comparison group, but selecting a single comparator state or hospital is inherently arbitrary and vulnerable to challenge. The Synthetic Control Method, introduced by Abadie and Gardeazabal and later formalized by Abadie, Diamond, and Hainmueller, resolves this by constructing a weighted composite of multiple untreated units that together reproduce the treated unit's pre-intervention trajectory far more closely than any single comparator could.
1. The Core Logic: A Data-Driven Counterfactual
Rather than selecting one comparison unit by clinical or geographic judgment, SCM uses an optimization algorithm to assign non-negative weights to a pool of untreated "donor" units so that the resulting weighted average — the synthetic control — matches the treated unit as closely as possible on pre-intervention outcomes and relevant predictor variables.
Once this synthetic control is constructed and validated against the pre-intervention period, it is projected forward through the post-intervention period. The gap between the treated unit's actual observed outcome and its synthetic counterfactual represents the estimated causal effect of the intervention. This approach transforms an inherently qualitative comparison choice into a transparent, reproducible, and quantifiable procedure.
2. Building the Donor Pool
The credibility of an SCM analysis depends heavily on the composition of the donor pool — the set of untreated units eligible to contribute weight to the synthetic control. Donor units should share the underlying structural and institutional characteristics of the treated unit and, critically, must not have been affected by the same intervention or a closely related spillover policy.
Researchers typically restrict the donor pool to units with reasonably similar baseline health system characteristics (comparable population size, similar insurance market structure, comparable regional healthcare infrastructure) to avoid extrapolating outside a sensible support region. Including a donor unit that was simultaneously exposed to a confounding policy change can silently bias the resulting synthetic trajectory.
3. Evidence Summary Table
| Standard / Methodology | Entity / Authority | Level of Evidence |
|---|---|---|
| Original SCM Framework | Abadie & Gardeazabal (2003) | High (Foundational Pillar) |
| Formal SCM Estimator | Abadie, Diamond & Hainmueller (2010) | High (Methodological Pillar) |
| Inference via Placebo Tests | Abadie, Diamond & Hainmueller (2015) | High (Statistical Standard) |
| Health Policy Application Guidance | AHRQ Comparative Effectiveness Research | High (Regulatory / Policy Standard) |
4. Weight Optimization and Predictor Selection
SCM weights are estimated by minimizing the discrepancy between the treated unit and the weighted donor composite across a set of pre-intervention predictor variables and outcome lags. This optimization is subject to two constraints that distinguish SCM from ordinary regression-based prediction: weights must be non-negative and must sum to one. These constraints prevent extrapolation beyond the observed range of the donor units and force the synthetic control to remain a genuinely interpretable "weighted average" of real comparison units rather than an unconstrained statistical projection.
Predictor selection should be informed by substantive health policy knowledge. For a Medicaid expansion evaluation, relevant predictors might include pre-period uninsured rates, hospital utilization patterns, and regional per-capita health expenditure. Poorly chosen predictors, or an over-reliance on outcome lags alone, can produce a synthetic control that fits the pre-period well by coincidence rather than by genuine structural similarity.
5. Validating Credibility: Placebo-in-Space and Placebo-in-Time
Because SCM typically involves a single treated unit, conventional standard errors and p-values are not directly applicable. Instead, the standard inferential approach is a placebo test. In a placebo-in-space test, the same SCM procedure is applied to every untreated donor unit as if each one had received the intervention. If the treated unit's post-intervention gap is unusually large relative to the distribution of "placebo gaps" from the donor units, this supports a genuine treatment effect rather than noise.
A placebo-in-time test artificially shifts the intervention date backward into the pre-intervention period. If the synthetic control produces a spurious "effect" even before the actual policy took place, this signals that the fitted model may be capturing pre-existing divergent trends rather than a true causal impact, undermining confidence in the primary result.
6. Actionable Steps: Implementing a Defensible SCM Analysis
| Step | Phase | Key Deliverable |
|---|---|---|
| Step 1 | Define the Treated Unit and intervention date precisely. | Study Design Specification |
| Step 2 | Assemble a Donor Pool free of confounding policy exposure. | Comparison Unit Set |
| Step 3 | Select Predictor Variables and outcome lags with domain justification. | Model Specification |
| Step 4 | Optimize Donor Weights and evaluate pre-intervention fit. | Synthetic Control Trajectory |
| Step 5 | Run Placebo-in-Space and Placebo-in-Time tests for inference. | Validated Causal Estimate |
7. Where SCM Excels in Health Policy Research
SCM is particularly well suited to evaluating state-level or system-level health policy changes: Medicaid expansion decisions made by individual states, hospital-level quality improvement mandates, regional public health campaigns, or national-level regulatory reforms. In each of these scenarios, the intervention is inherently applied to a single aggregate unit, making SCM's donor-pool weighting approach far more defensible than an arbitrarily chosen single comparator, and considerably more transparent than an unweighted panel regression that implicitly assumes uniform comparability across all untreated units.
Elevate Your Health Policy Research with Lingcore SCI Tools
Constructing a credible synthetic control requires careful donor pool curation, transparent weight reporting, and rigorous placebo testing. Lingcore SCI provides specialized AI-driven tools to strengthen your causal policy evaluation:
- Paper Analyzer: Audit your SCM manuscript for donor pool justification, predictor selection, and placebo test completeness.
- Review Builder: Generate structured literature reviews on quasi-experimental health policy evaluation methods with verified citations.
- Journal Matcher: Find the health policy and health economics journals that prioritize rigorous synthetic control applications.
Conclusion
The Synthetic Control Method transforms one of the most persistent challenges in health policy evaluation — the absence of a natural comparison group for a single treated jurisdiction — into a transparent, data-driven exercise. By replacing arbitrary comparator selection with an optimized donor-pool weighting scheme, and by subjecting results to rigorous placebo testing, researchers can defend causal claims about policy interventions that would otherwise rest on subjective judgment alone. As administrative health datasets continue to expand across states and health systems, the Synthetic Control Method is positioned to remain an indispensable tool for evaluating the real-world impact of health policy throughout 2026 and beyond.