 LINGCORE SCI
LINGCORE SCI
Regression Discontinuity Design: A Causal Inference Framework for Health Policy Research
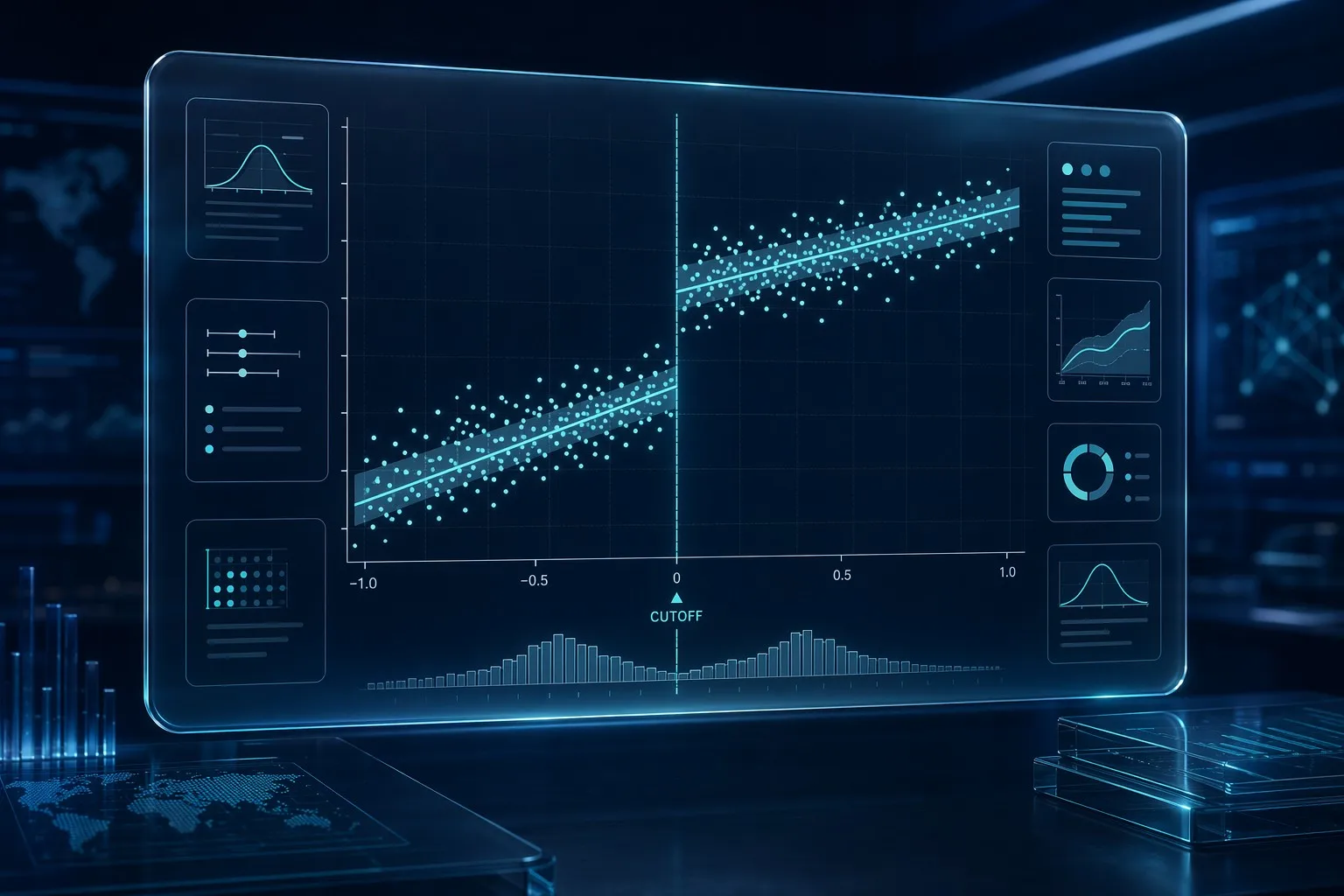
Regression Discontinuity Design (RDD) exploits a threshold-based eligibility rule (e.g., age, income, or a clinical risk score) to estimate a local causal effect at the cutoff. Units just above and below the threshold are assumed comparable, allowing researchers to approximate randomized controlled trial (RCT) conditions without an actual randomization process.
Health policy interventions rarely apply uniformly. Medicare eligibility begins precisely at age 65. A hospital triage protocol activates only when a severity score crosses a fixed point. A subsidized screening program is limited to patients below a specific income threshold. These arbitrary, rule-based cutoffs create a natural experiment that Regression Discontinuity Design (RDD) is uniquely equipped to exploit.
Unlike propensity score methods, which attempt to balance covariates across an entire observational sample, RDD narrows its causal claim to a single point: the threshold itself. This narrower scope is precisely what gives RDD its methodological strength. When correctly specified, RDD estimates are considered among the most credible non-experimental causal estimates available to health policy researchers, frequently cited alongside RCTs in evidence hierarchies for policy evaluation.
1. The Core Logic: Local Randomization at the Cutoff
The foundational assumption of RDD is that individuals cannot precisely manipulate their position relative to the threshold. A patient whose age is 64 years and 364 days differs from a patient who is 65 years and 1 day old only by the passage of time, not by any systematic clinical or behavioral distinction. Under this assumption, the assignment to "treatment" (Medicare-eligible) versus "control" (not yet eligible) is as good as random in the immediate neighborhood of the cutoff.
This is the central insight that separates RDD from typical observational designs. Researchers are not attempting to control for confounding across a heterogeneous population; they are comparing two nearly identical groups that differ only by which side of an arbitrary line they fall on. The causal estimate produced is a Local Average Treatment Effect (LATE) — valid at the cutoff, not necessarily generalizable to the full population.
2. Sharp RDD vs. Fuzzy RDD
RDD applications split into two distinct structural categories, and identifying the correct type is the first decision point in any RDD-based manuscript.
- Sharp RDD: Treatment assignment is a deterministic function of the running variable. Every unit above the cutoff receives treatment; every unit below does not. Medicare eligibility at age 65 is a canonical sharp RDD scenario.
- Fuzzy RDD: The probability of treatment jumps discontinuously at the cutoff but does not go from 0% to 100%. This occurs when clinical guidelines recommend, but do not mandate, an intervention above a risk threshold, and physician discretion or patient non-compliance blurs the assignment. Fuzzy RDD requires an instrumental variable approach, using the threshold-crossing indicator as the instrument for actual treatment receipt.
3. Evidence Summary Table
| Standard / Methodology | Entity / Authority | Level of Evidence |
|---|---|---|
| RDD Foundational Framework | Thistlethwaite & Campbell (1960) | High (Methodological Pillar) |
| Local Linear / Bandwidth Theory | Imbens & Kalyanaraman (2012) | High (Statistical Pillar) |
| AHRQ Comparative Effectiveness Guidance | Agency for Healthcare Research and Quality | High (Regulatory / Policy Standard) |
| Quasi-Experimental Reporting | TREND Statement | High (Reporting Standard) |
4. Verifying the Key Assumption: No Manipulation of the Running Variable
The entire causal argument of RDD collapses if participants can precisely manipulate their score to land on the favorable side of the cutoff. If patients or providers know that crossing a specific lab value triggers an expensive intervention, and providers round borderline values upward to secure treatment for their patients, the local randomization assumption is violated.
The standard diagnostic for this threat is the McCrary density test, which examines whether there is a statistically significant discontinuity in the density of the running variable at the cutoff itself. A smooth, continuous density supports the validity of the design; a visible jump in density at the threshold is a red flag for manipulation and is one of the most common reasons RDD manuscripts face methodological rejection.
5. Bandwidth Selection and Functional Form
Because RDD estimates a local effect, the choice of how much data around the cutoff to include — the bandwidth — directly determines the bias-variance tradeoff. A narrow bandwidth reduces bias (the comparison groups are more similar) but increases variance (fewer observations, less statistical power). A wide bandwidth does the opposite.
Modern RDD practice, following the data-driven optimal bandwidth selection procedures developed by Imbens and Kalyanaraman, and later refined by Calonico, Cattaneo, and Titiunik (the CCT / rdrobust framework), requires researchers to report results using the automatically selected optimal bandwidth alongside sensitivity analyses at half and double that bandwidth. Reviewers increasingly expect local linear regression rather than high-order polynomial fits, since high-order polynomials are prone to overfitting near the boundary and can produce spurious discontinuities.
6. Actionable Steps: Implementing a Defensible RDD Analysis
| Step | Phase | Key Deliverable |
|---|---|---|
| Step 1 | Confirm the Running Variable and cutoff are pre-determined and not manipulable. | Design Justification |
| Step 2 | Classify the design as Sharp or Fuzzy RDD. | Model Specification |
| Step 3 | Run the McCrary Density Test for manipulation. | Validity Diagnostic |
| Step 4 | Select Optimal Bandwidth via data-driven methods (rdrobust). | Analytical Plan |
| Step 5 | Report Local Average Treatment Effect with robust/bias-corrected CIs. | Final Effect Estimate |
7. Where RDD Excels in Medical Research
RDD is particularly well suited to health systems research because clinical and administrative rules are inherently full of thresholds. Common applications include evaluating the effect of Medicare enrollment at age 65 on hospitalization rates, assessing ICU admission protocols triggered by a specific severity score, measuring the impact of income-based subsidy cutoffs on preventive screening uptake, and analyzing guideline-based treatment thresholds such as statin initiation at defined LDL cholesterol levels.
In each of these cases, a standard observational comparison across the full population would be confounded by the very factors that determine eligibility. RDD sidesteps this problem entirely by concentrating the causal comparison on the narrow window where treatment assignment is effectively arbitrary.
Elevate Your Causal Inference Research with Lingcore SCI Tools
Designing and reporting a defensible RDD study requires precise attention to bandwidth selection, manipulation testing, and functional form. Lingcore SCI provides specialized AI-driven tools to strengthen your quasi-experimental research:
- Paper Analyzer: Audit your RDD manuscript against current quasi-experimental reporting standards and identify bandwidth or specification vulnerabilities.
- Review Builder: Generate structured literature reviews on threshold-based causal inference methods with verified citations.
- Journal Matcher: Find the high-impact health policy and biostatistics journals that prioritize rigorous quasi-experimental designs.
Conclusion
Regression Discontinuity Design occupies a distinctive position in the causal inference toolkit: it does not require the researcher to control for every possible confounder, only to defend the assumption that assignment near the cutoff is effectively random. This makes RDD an exceptionally credible design for evaluating the vast number of policies, guidelines, and eligibility rules that govern modern health systems. As data-driven bandwidth selection and robust inference procedures continue to mature, RDD is positioned to remain one of the most persuasive quasi-experimental methods available to health policy researchers throughout 2026 and beyond.