 LINGCORE SCI
LINGCORE SCI
Quantile Regression in Clinical Research: Beyond Average Treatment Effects
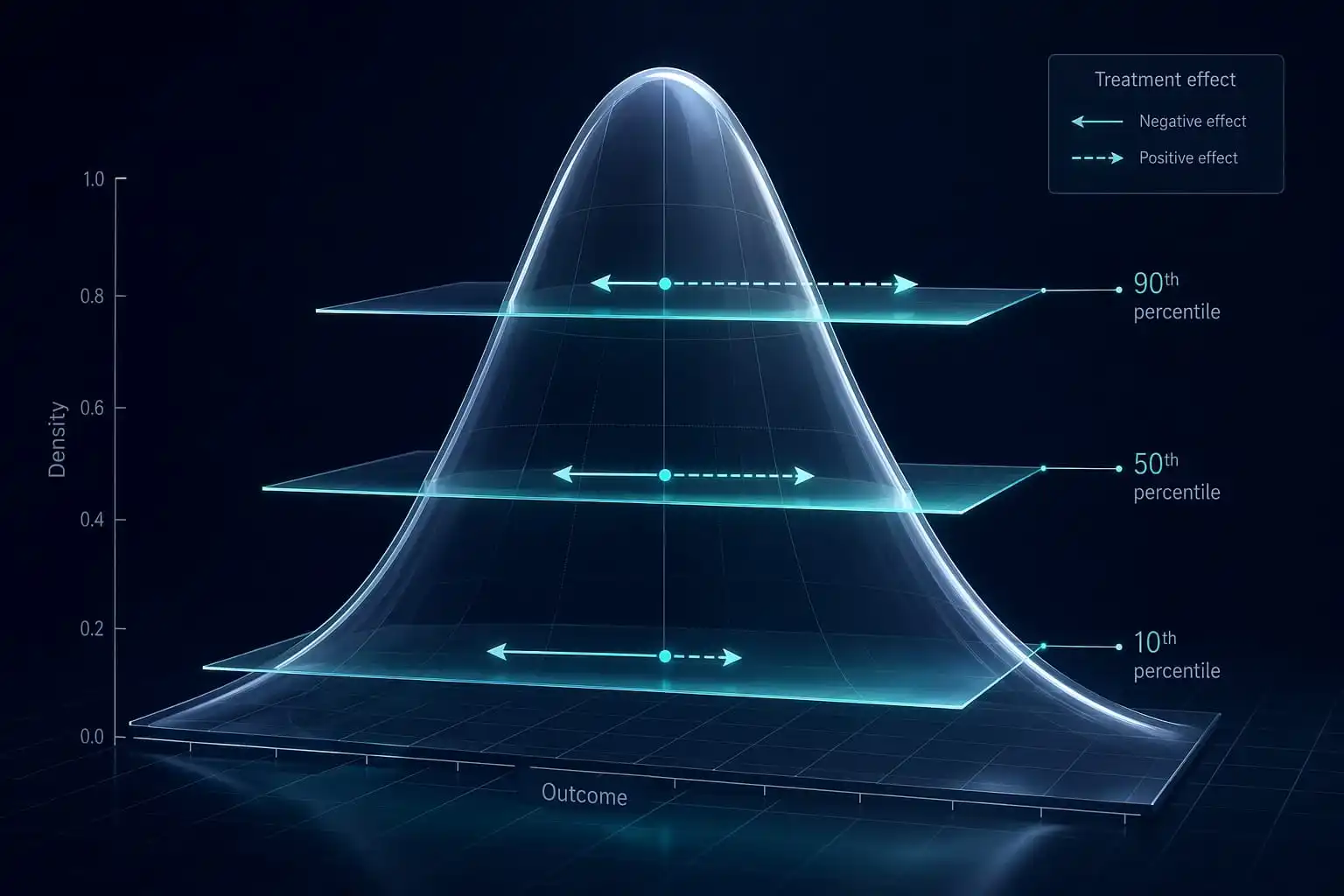
Quantile regression models the effect of an exposure or treatment on specific percentiles of an outcome distribution (e.g., the 10th, 50th, 90th), rather than only the conditional mean estimated by ordinary least squares. It reveals heterogeneous treatment effects — a drug may show no effect at the median but a substantial effect at the distribution's tails, information a mean-based model cannot detect.
Ordinary least squares (OLS) regression and its clinical cousins answer a narrow question: what happens to the average patient? But average effects can conceal clinically important heterogeneity. A lipid-lowering therapy might produce a modest average reduction in LDL cholesterol while delivering a dramatically larger reduction among patients who start with the highest baseline levels — precisely the patients for whom intervention matters most. A mean-based model, by construction, cannot see this pattern.
Quantile regression, introduced by Koenker and Bassett in 1978, provides a complete picture of how a covariate shifts the entire conditional distribution of an outcome, not merely its center. In an era of precision medicine, where the clinical relevance of a treatment effect often depends on where a patient sits within the outcome distribution, quantile regression has moved from a statistical curiosity to a standard tool in biomarker research, health economics, and growth curve analysis.
1. The Core Logic: Modeling the Whole Distribution
OLS regression estimates a single line describing how the mean of the outcome changes with a covariate, minimizing the sum of squared residuals. Quantile regression instead estimates a family of lines, each describing how a specific quantile of the outcome changes with the same covariate, by minimizing an asymmetrically weighted sum of absolute residuals — a loss function that assigns different weights to positive and negative residuals depending on the quantile being estimated.
The result is a conditional quantile function that can look completely different from the conditional mean function. Two datasets can share an identical average treatment effect while having a treatment effect of zero at the median and a large effect at the 90th percentile, or vice versa. Only quantile regression can distinguish between these fundamentally different clinical realities.
2. Why the Mean Can Mislead in Clinical Data
Clinical outcome distributions are frequently skewed, heavy-tailed, or bimodal — length of hospital stay, healthcare costs, biomarker concentrations, and time-to-recovery measures rarely follow a symmetric bell curve. In such distributions, the mean is disproportionately influenced by a small number of extreme observations and may not represent any clinically meaningful patient experience at all.
Quantile regression is also inherently robust to outliers because it is based on absolute rather than squared deviations, making it particularly well suited to biomarker and cost data where a handful of extreme values would otherwise distort an OLS-based conclusion. This robustness, combined with its ability to reveal distributional heterogeneity, makes quantile regression a natural complement to — not merely an alternative to — standard mean-based analysis.
3. Evidence Summary Table
| Standard / Methodology | Entity / Authority | Level of Evidence |
|---|---|---|
| Original Quantile Regression Framework | Koenker & Bassett (1978) | High (Foundational Pillar) |
| Quantile Regression Textbook Standard | Koenker (2005), Cambridge University Press | High (Methodological Standard) |
| Growth Reference Charts Application | WHO Child Growth Standards | High (Regulatory / Clinical Standard) |
| Health Economics Application Guidance | ISPOR Health Economics Guidelines | High (Applied Methodology Standard) |
4. Interpreting Quantile Coefficients
A quantile regression coefficient at the 0.5 quantile (the median) is interpreted similarly to a robust version of the OLS coefficient — the change in the median outcome per unit change in the covariate. Coefficients at other quantiles carry a distinct interpretation: the coefficient at the 0.9 quantile describes the effect specifically among patients whose outcome values fall near the top of the distribution, holding other covariates constant.
Plotting the estimated coefficient against the quantile level, with a confidence band, is the standard way to communicate results. A flat line across all quantiles suggests the covariate has a uniform, location-shift effect — consistent with what OLS alone would suggest. A sloped or non-monotonic line reveals genuine distributional heterogeneity that a single mean-based coefficient would have concealed entirely.
5. Applications in Growth Curves and Biomarker Reference Ranges
Quantile regression is the statistical backbone of modern pediatric growth charts, including the WHO Child Growth Standards, precisely because clinical growth assessment requires knowing where an individual child falls relative to age-specific percentile curves — not merely whether that child differs from an average trend. The same logic extends naturally to biomarker reference range construction, where clinicians need percentile-specific thresholds (e.g., the 5th and 95th percentiles of a lab value by age and sex) rather than a single population mean and standard deviation, particularly when the underlying biomarker distribution is skewed.
6. Actionable Steps: Applying Quantile Regression to Clinical Data
| Step | Phase | Key Deliverable |
|---|---|---|
| Step 1 | Examine the outcome distribution for skewness, heavy tails, or bimodality. | Distributional Diagnostic |
| Step 2 | Select clinically meaningful quantiles (e.g., 10th, 50th, 90th). | Quantile Specification |
| Step 3 | Fit separate quantile regression models for each selected quantile. | Conditional Quantile Estimates |
| Step 4 | Construct bootstrapped confidence intervals for each coefficient. | Uncertainty Quantification |
| Step 5 | Plot the coefficient-by-quantile curve to assess heterogeneity. | Distributional Effect Profile |
7. Reporting Quantile Regression in Manuscripts
Reviewers evaluating a quantile regression analysis expect explicit justification for the chosen quantiles, a clear statement of whether findings were pre-specified or exploratory, and reporting of results at multiple quantiles rather than a single favorable one that could reflect selective reporting. Presenting the full coefficient-by-quantile plot alongside the traditional mean-based estimate gives readers the complete picture and preempts a common and reasonable reviewer critique: that a single quantile result, in isolation, is difficult to distinguish from noise.
Elevate Your Biostatistical Research with Lingcore SCI Tools
Applying quantile regression correctly requires careful quantile selection and transparent reporting of distributional heterogeneity. Lingcore SCI provides specialized AI-driven tools to strengthen your clinical manuscript:
- Paper Analyzer: Audit your quantile regression methodology and reporting completeness against current biostatistical standards.
- Review Builder: Generate structured literature reviews on distributional regression methods with verified citations.
- Journal Matcher: Identify biostatistics and precision medicine journals that value distributional treatment effect analysis.
Conclusion
Average treatment effects are a convenient summary, but they are not the whole clinical story. Quantile regression restores the information that mean-based models discard, revealing whether an intervention benefits everyone equally or concentrates its impact among patients at the extremes of the outcome distribution — precisely the patients most likely to shape a treatment decision. As precision medicine continues to demand more granular evidence about who benefits and by how much, fluency in quantile regression is becoming an increasingly valuable skill for researchers publishing in biomarker science, health economics, and clinical epidemiology through 2026.